- How do I know if breast augmentation is a good option for me?
- Breast augmentation is the second most common cosmetic surgery after liposuction. Those who would benefit the most are those who desire an increase in breast size, or to restore breast shape after postpartum deflation. Other common reasons are to correct breast asymmetry, enhance breast shape and volume, and improve fitting in clothing.
- Are there any reasons why I would not qualify for breast augmentation?
- You must be nicotine free for 4 weeks before and after surgery. Patients requiring anticoagulation are generally not candidates.
- You must be older than 18 years for breast augmentation and older than 22 years for use of silicone implants
- What’s better, silicone or saline? Also, my friend has “gummy bear” implants, should I get those?
- The advantage of silicone implants are they feel more natural and look more natural than saline. Saline implants can wrinkle and thus look and feel less natural. On the other hand, ruptured silicone implants can be difficult to detect and can cause local inflammation resulting in granulomas. Therefore, the FDA recommends MRI 3 years after surgery and every 2 years thereafter for silicone implants to monitor for undetected leaks or ruptures. If a saline implant leaks or ruptures, the saline is safely absorbed by the body.
 2
2
-
- Gummy bear implants, also known as shaped or textured implants, were designed to decrease the rate of capsular contracture associated with breast implants. There is evidence that links these implants in rare case to a lymphoma known as anaplastic large cell lymphoma (ALCL). Recent hearings by the FDA confirmed these findings. Due to the low but present risk of associated lymphoma, it is our practice’s policy not to use textured implants.
- How do I know what sized implants to choose?
- Implant size is based upon the patient’s goals in terms of desired breast size and projection. The implant size is limited by the measured patient’s breast base width. These goals are discussed with a board-certified plastic surgeon who will offer what implants sizes are possible in coordination with patient safety. Choosing implants that are too large has unwanted consequences of stretching the tissues and potentially causing rippling, palpability of the implant, and atrophy of the breast skin and tissue.
- Where will my scar be?
- Generally, our practice utilizes a scar in the fold of the breast otherwise known as the inframammary crease. This allows for a well-hidden scar and that allows for best control of the implant placement.
- There are other options but they carry greater risk and limitations. The peri-areolar scar has a higher rate of infection, problematic scarring and nipple sensitivity changes. The transaxiilary scar can have a higher revision rate due to difficulty in proper placement of the implants. The transumbilical scar is limited by only the use of saline implants.
- Will the implant be placed above or below the muscle?
- This question is in reference to if the implant is placed above or below the pectoralis muscle, also known as subpectoral (below the muscle) versus subglandular (above the muscle).
- Subpectoral is the most common method for implant placement. Its major advantage is that it has minimal interference with mammogram screenings for detection of breast cancer. Its disadvantage is in patients who have a muscular chest because flexion of the pectoralis muscle can cause visible rippling of the implant known as animation deformity.
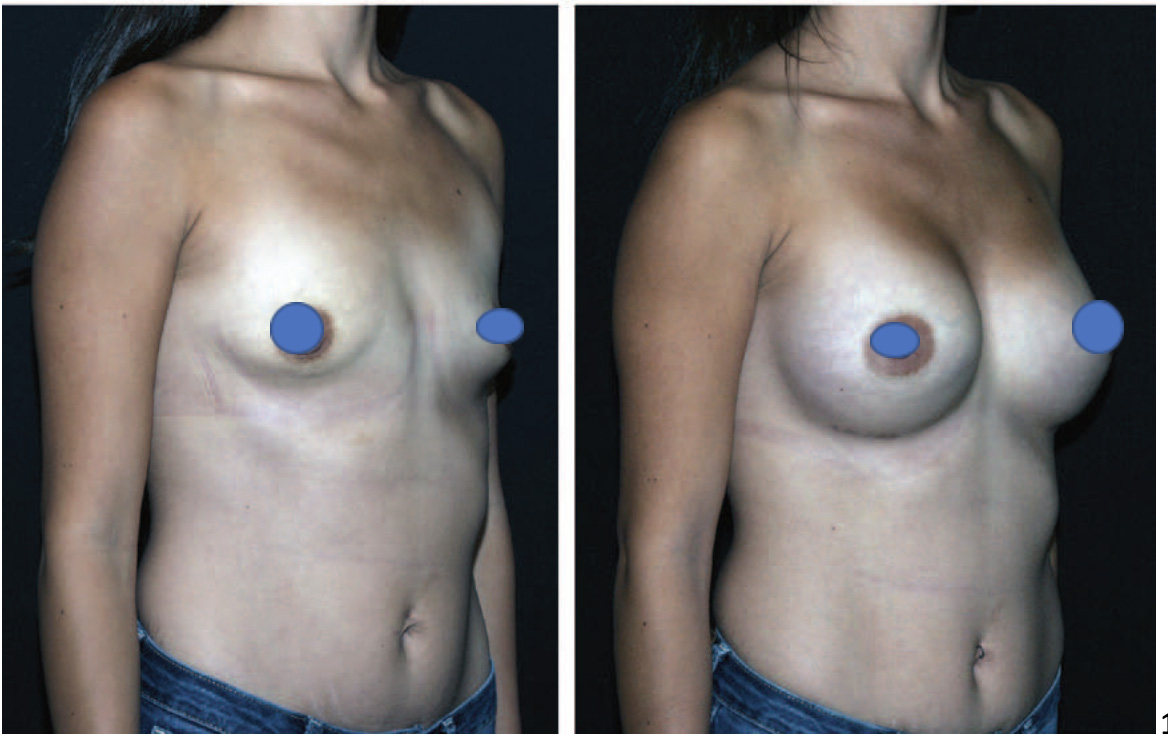
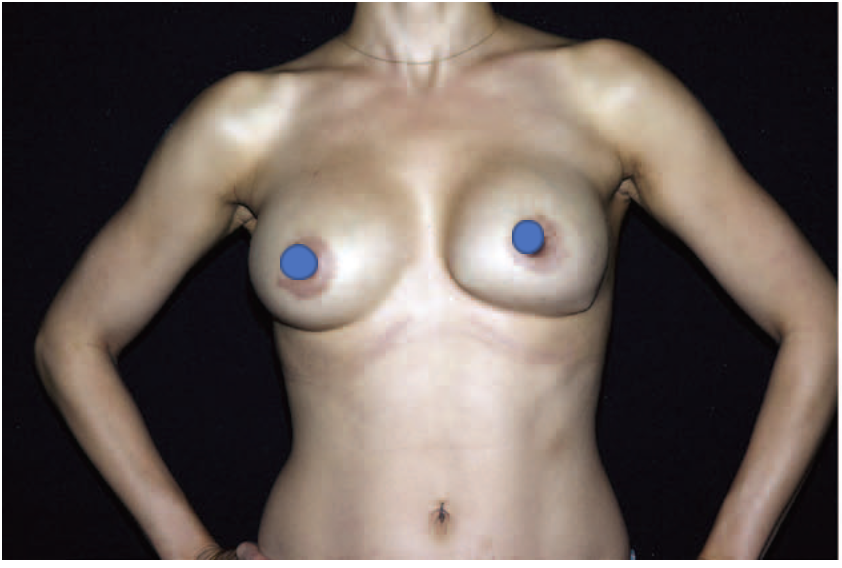
2 – subpectoral augmentation
-
- Subglandular placement has the advantage of avoiding animation deformity. However, it does have a higher rate of capsular contracture, more implant wrinkling and palpability, and it can interfere with mammogram detection of breast cancer.
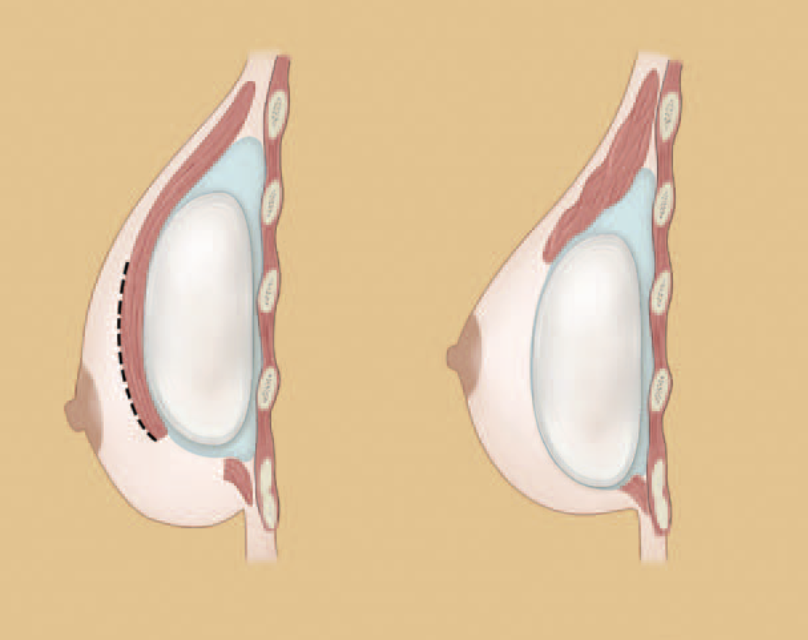
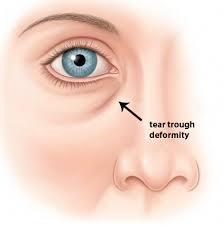
4 – animation deformity
- Will I need a breast lift at the same time?
- A breast lift is known as a mastopexy. In combination with augmentation it is known as augmentation mastopexy. Common indications for needing a lift with augmentation include postpartum atrophy of the breasts with associated ptosis, if the nipple position is below the level of the breast fold, massive weight loss patients, or if there is no visible skin below the areola when viewed in a standing position. The decision for a lift in combination with an augmentation should be made in coordination and discussion with a board-certified plastic surgeon.
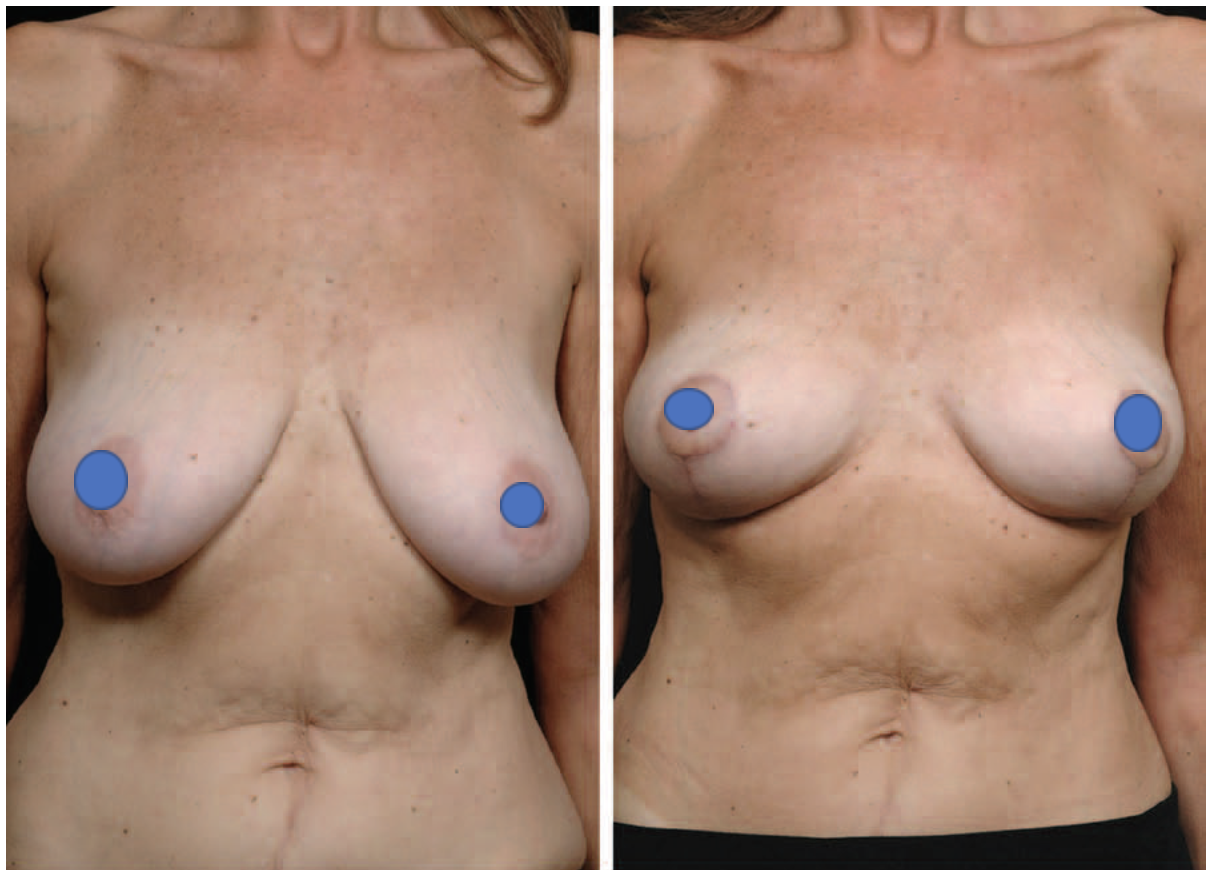
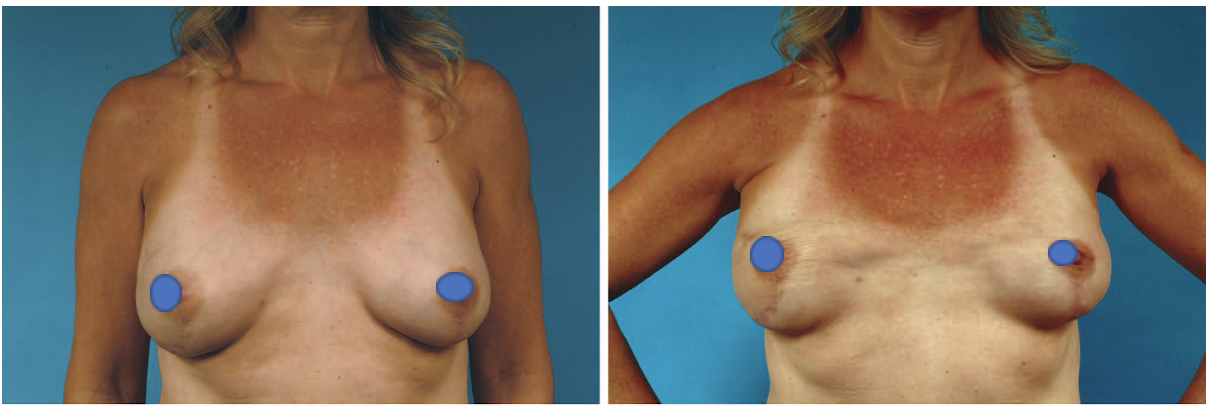
3 – breast lift with implant – augmentation mastopexy
- What are the complications associated with this surgery?
- 15% of patients have altered nipple sensation
- Infection rate is low at < 1%, as is risk of hematoma
- Saline implants leak at a rate of 1% per year. Silicone leak rates incidence is difficult to assess. Some studies cite 30% at 5 years. For this reason, the FDA recommends MRI surveillance for leaks/ruptures with silicone implants. If found, a discussion with a board-certified plastic surgeon is necessary to discuss removing the implants and possibly the capsule, and replacing the implants.
- There is the possibility of need for reoperation or revision – 20% rate over 3 years. The most common reason for revision is size change.
- The long-term risk associated with implants is the phenomenon known as capsular contracture. This is where the human body forms a capsule around any foreign object present within soft tissue. Over many years the capsule formed can become hard and even calcified. In some cases, the firm capsule can result in pain or distortion of the breast. In those cases, removal of the implant and capsule is needed along with replacement of the implant.
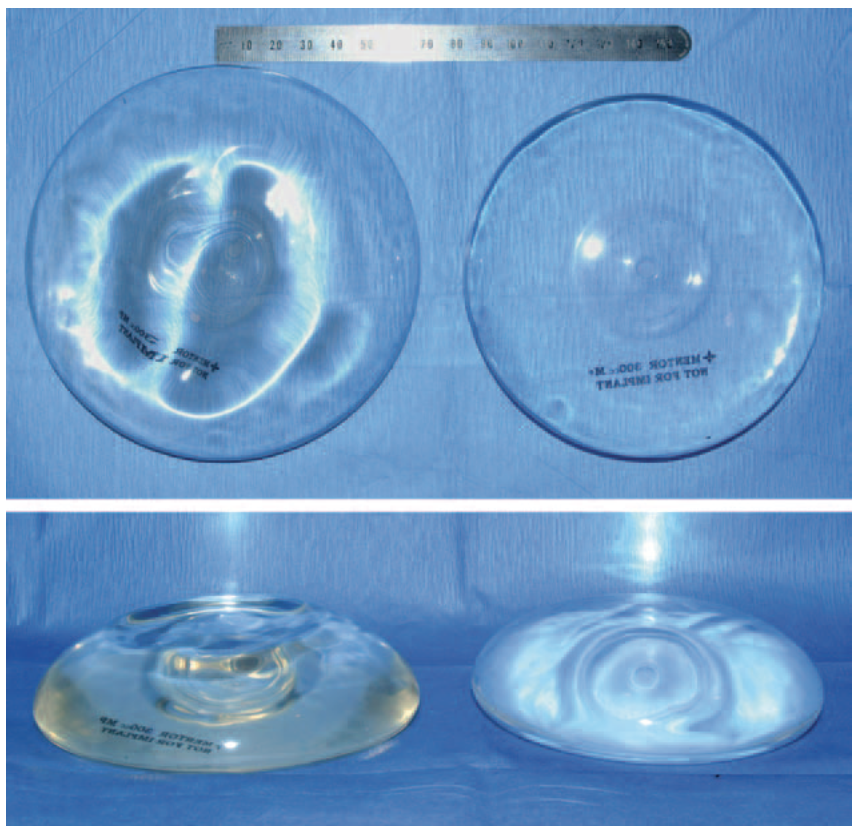
1 – left breast capsular contracture
- After surgery, when can I start exercising again and when can I return to work?
- Ok to commence aerobic activity and exercise at 2 weeks. Ok to start exercising with weights at 6 weeks. Until then, no lifting more than 5 lbs.
- Ok to return work after 3 days. Ok to drive 24 hours after surgery
- Any other limitations?
- No underwire bra for 6 weeks, wireless bras only
- How can I learn more and schedule a consultation?
- Call (205) 871-4440 to schedule a consultation with one of our board-certified plastic surgeons to discuss more regarding breast augmentation. Our office is located at 2850 Cahaba Road, Birmingham, Alabama 35223
References
- Schwartz, Michael. “Evidence-Based Medicine: Breast Augmentation.” Plastic and Reconstructive Surgery Journal. CME. July 2017.
- Hidalgo, David; Spector, Jason. “Breast Augmentation.” Plastic and Reconstructive Surgery Journal. CME. April 2014.
- Hidalgo, David; Spector, Jason. “Mastopexy.” Plastic and Reconstructive Surgery Journal. CME. October 2013.
4. Hammond, Dennis C; Schmitt, William P.; O’Connor, Elizabeth A. “Treatment of Breast Animation Deformity in Implant-Based Reconstruction with Pocket Change to Subcutaneous Position.” Plastic and Reconstructive Surgery Journal. Vol. 135, Number 6, June 2015.










 A “tummy tuck” is a cosmetic surgery that involves rejuvenation of the abdomen and flanks. Your plastic surgeon may also refer to this procedure as an abdominoplasty. There are three major components of a tummy tuck – management of excess skin, contouring of excess fat, and tightening of the abdominal muscles.
A “tummy tuck” is a cosmetic surgery that involves rejuvenation of the abdomen and flanks. Your plastic surgeon may also refer to this procedure as an abdominoplasty. There are three major components of a tummy tuck – management of excess skin, contouring of excess fat, and tightening of the abdominal muscles.